Navigating Wisdom Tooth Extraction in London: A Clinical Guide to Third Molars
Wisdom tooth extraction in London becomes medically necessary when a patient’s jaw lacks the spatial capacity to accommodate the third molars, leading to partial eruption, impaction, or the crowding of adjacent healthy teeth.
The optimal window for assessment and removal is between the ages of 17 and 25, when the roots are not yet fully formed and the surrounding bone is less dense, allowing for a safer procedure and a significantly faster, less complicated recovery.
For young adults living in Southwestern Ontario, the emergence of third molars is an evolutionary rite of passage that often brings localized pain, swelling, and frustration. Unlike other dental procedures that can be delayed, problematic wisdom teeth operate on their own unpredictable timeline.
Because London is a major educational hub—home to tens of thousands of students at Western University and Fanshawe College—the local demographic heavily skews toward the exact age group most affected by wisdom tooth complications.
Managing this aspect of oral health requires understanding the biology of impaction, recognizing the early warning signs of infection, and utilizing modern diagnostic imaging to plan a safe, predictable extraction.
The Biology of the Third Molar
To understand why these teeth cause so much trouble, we have to look at human anatomy. Our ancestors required a third set of molars to grind down a tough, coarse diet of raw roots, leaves, and meats. Over millennia, as human diets softened with the advent of cooking and agriculture, our jawbones gradually became smaller.
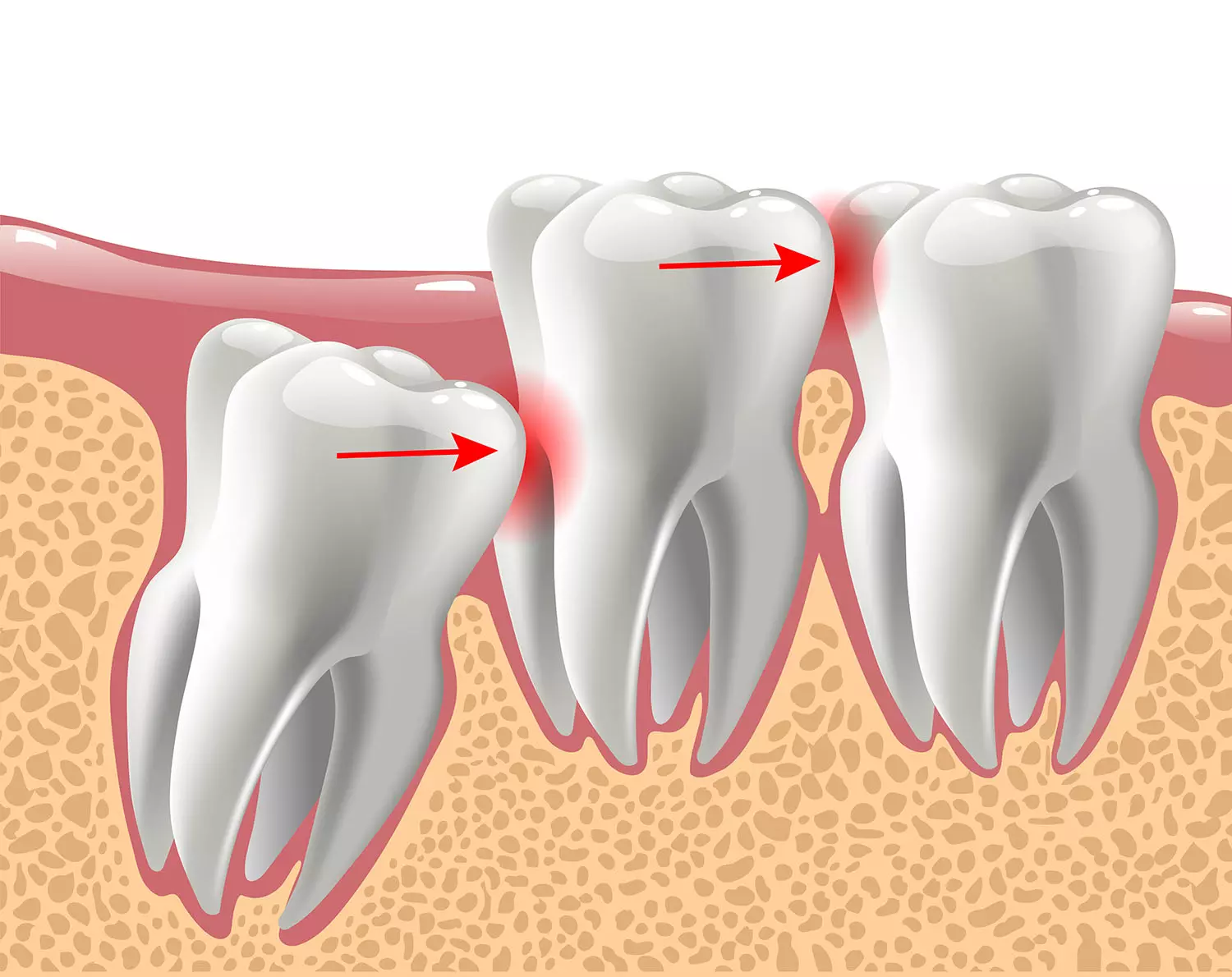
However, our genetics still program the development of 32 teeth. When those final four molars attempt to erupt into a jaw structure designed to comfortably hold only 28, a spatial conflict occurs. This lack of room prevents the teeth from emerging vertically and functioning properly, resulting in a condition known as impaction.
Types of Wisdom Tooth Impaction
Not all wisdom teeth behave the same way. The angle at which the tooth is trapped beneath the gum line dictates the complexity of the extraction:
- Mesial Impaction: The most common variation. The tooth is angled forward, pushing directly against the second molar.
- Vertical Impaction: The tooth is oriented straight up but remains trapped beneath the jawbone or gum tissue because there is simply no space to break through.
- Horizontal Impaction: The tooth is entirely sideways, growing at a 90-degree angle into the roots of the adjacent teeth. This often requires more advanced surgical intervention.
- Distal Impaction: The rarest form, where the tooth is angled backward toward the rear of the jaw.
When to Wait and When to Act
A common misconception is that all wisdom teeth must be removed. If the third molars erupt fully, align perfectly with the opposing teeth, and can be easily reached with a toothbrush and floss, they can often be left alone. However, this ideal scenario is rare.
For the vast majority of patients, partial eruption creates a flap of gum tissue (an operculum) over the tooth. This flap acts as a trap for food debris and bacteria. Because it is nearly impossible to keep this deep pocket clean, it frequently leads to pericoronitis—a painful, acute localized infection of the gums.
Symptoms that indicate an immediate need for an evaluation include:
- Radiating pain in the back of the jaw or temporomandibular joint (TMJ).
- Swelling and redness in the gums behind the second molars.
- A persistent bad taste or odor in the mouth, indicating trapped bacteria.
- Difficulty opening the mouth fully (trismus).
For university students and young professionals managing tight schedules, waiting until a tooth is actively infected to seek help is a strategic error. Active infections can reduce the efficacy of local anesthetics and complicate the healing process.
Scheduling a proactive third molar assessment in the Forest City allows you to address the issue on your own timeline—like during a reading week or summer break—rather than during midterms.
Modern Diagnostics: The Role of 3D Imaging
The standard of care for planning an extraction has evolved significantly. In the past, dentists relied exclusively on 2D panoramic X-rays. While useful for a broad overview, a 2D image flattens complex anatomy, making it difficult to determine the exact distance between the wisdom tooth roots and critical structures like the inferior alveolar nerve (which supplies sensation to the lower lip and chin).
Today, modern clinics utilize Cone Beam Computed Tomography (CBCT). A CBCT scan captures a high-resolution, 3D topographical map of your entire jaw.
This technology allows the clinical team to rotate the image, slice it digitally, and measure the proximity of the tooth roots to the nerve canal and the maxillary sinus cavity down to the millimeter.
By eliminating the guesswork, 3D imaging allows local dental professionals who manage complex extractions to design a precise, minimally invasive surgical pathway. This translates directly to smaller incisions, less bone removal, and a dramatically more comfortable recovery for the patient.
Read: Family Dentistry in London, Ontario: A Practical Guide
The Recovery Phase: Timeline and Best Practices
The success of a wisdom tooth extraction depends as much on the patient's postoperative care as it does on the surgeon's skill. The mouth is a remarkably fast-healing environment, but the initial 72 hours are critical for establishing a healthy blood clot in the empty socket.
Days 1 to 3: The Crucial Window
Immediately following the procedure, localized swelling and mild to moderate discomfort are standard physiological responses.
- Swelling Control: Apply ice packs to the outside of the face (20 minutes on, 20 minutes off) for the first 48 hours to minimize inflammation.
- Dietary Adjustments: Stick exclusively to cool, smooth liquids and soft foods. Think protein shakes, Greek yogurt, applesauce, and lukewarm broth. Avoid anything hot, spicy, or textured (like seeds or nuts) that could become lodged in the surgical site.
- The Golden Rule: Do not use a straw, spit forcefully, or smoke. The negative pressure created in the mouth by these actions can dislodge the fragile blood clot, exposing the underlying bone and nerves.
Preventing Dry Socket
Dislodging the blood clot leads to a condition called alveolar osteitis, commonly known as "dry socket." It is characterized by an intense, radiating, throbbing pain that typically begins on the third or fourth day post-surgery.
While relatively uncommon (occurring in roughly 2% to 5% of routine extractions), the risk increases significantly for patients who smoke or fail to follow soft-diet protocols. If you experience this sharp increase in pain after the initial healing days, contact your clinic immediately; the site can be quickly dressed with a medicated paste to provide near-instant relief.
Days 4 to 7: Transitioning Back to Normal
By the end of the first week, the swelling should largely subside, and you can begin slowly reintroducing more solid foods—like pasta, scrambled eggs, and soft fish. You will also be instructed to gently irrigate the lower sockets with a curved plastic syringe filled with warm salt water to keep the healing sites free of food debris.
Securing Your Long-Term Oral Health
Wisdom teeth are notorious for acting up at the most inconvenient times. Whether you are a local London resident noticing a dull ache in your jaw, or a parent whose teenager is approaching their late teens, early diagnostic imaging is the most effective preventative tool available.
By evaluating the trajectory of the third molars before they breach the surface, you can avoid the pain of impaction, protect the alignment of the surrounding healthy teeth, and ensure the structural integrity of your smile for the future.